Pulmonary Function Studies
Diffusion Capacity
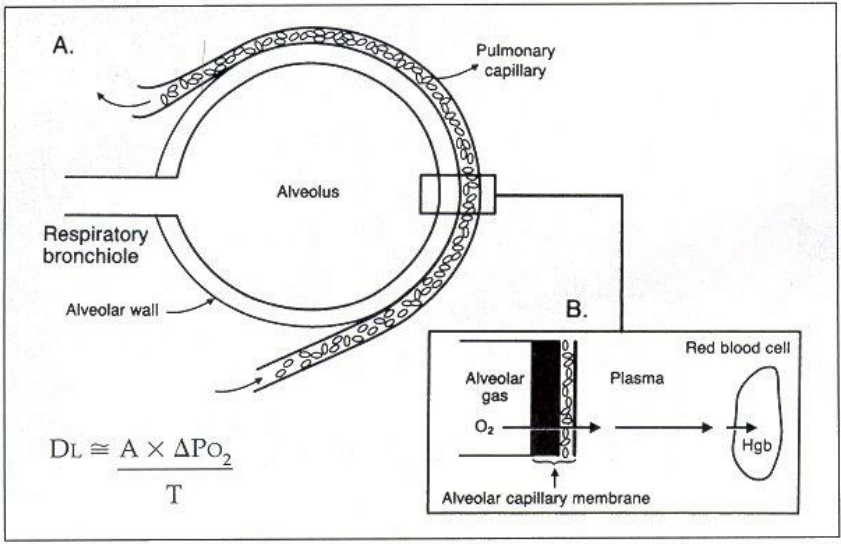
The final component of the full PFT exam is the measurement of Duffusion Capacity of Carbon Monoxide (DLco). Due to its rich capillary bed associated with the large surface area of the alveoli, the lung is very efficient at oxygen delivery and CO2 extraction. In addition given the presence of hemoglobin binding of oxygen there is alway a concentration gradient for the movement of oxygen across the aveolar membrane. The DLco maneuver is simialr to nitrogen washout in that at FRC the patient is switch from breathing room air to a bag containing a low but known concentration of carbon monixide. The patient is instructed to perform an inspiratory capacity maneuver and hold that breath for 10 seconds then exhale to residual volume. If there are issues with the transfer of CO, there will be more CO in the exhaled breath indicating diffusion impairment. CO is chosen since its affinity for Hemoglobin is 100 times higher than oxygen, therefore the absorption is not flow but diffusion limited.
Based on the physiology of CO absorption what conditions do you feel would be associated with a reduction of DLco.
By Including a small amount of an inert gase (helium), and again utilizing Boyles Law we can calculate alveolar volume (Va) and an assessment and potential correction tool for the DLco value.
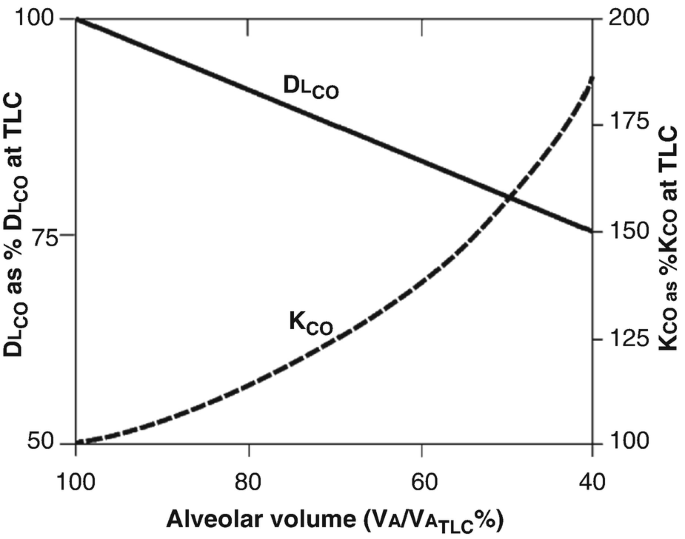
As it was explained to me in an overly simplistic way, if you have a healthy person who undergoes a pneumonectomy, the DLco will be reduced from the removal of one lung. The Va should be 50% of the prepneumonectomy value, therefore the corrected value for the diffusion capacity adjusted for alveolar volume (DLco/Va) would be normal.
Because the relationship between the Va and DLco is much more complex than a proportional reduction, substituting the DLco/Va for the determination of diffusional impairment is controversial and not advised. But given the impact of the inspiratory volume on the degree of CO absorption the use of only the raw value of DLco is also fraught. My approach is to use the Va as a quality control measure. If Va is similar to the precent predicted ideally for IC, but secondarily FVC or TLC, the DLco is a reasonable measure of diffusional impairment. If Va is 5-10% less than these parameters I include a proviso that a portional of the reduction in DLco is due to technical factors.
Combine this with the impact of when the technician switches to the DLco bag, the depth of inspiration, the time of inspiration, potential mouth leaks and the adequacy of exhalation the day to day variation of DLco can be as much as 20-25%.
Therefore the ranges for impairment are much more broad and less reliable than for spirometry:
| Dlco % Predicted | Impairment | Z-score |
|---|---|---|
| > 80% | Normal | < 1.64 |
| 60-80% | Mild | 1.64 - 2.5 |
| 50-60% | Moderate | 2.5 - 3.5 |
| 40-50% | Moderately Severe | 3.5 - 4.5 |
| <40% | Severe | > 4.5 |
What conditions can result in an abnormally high DLco?